In 1895, the German physicist Röntgen took the world's first X-ray film using his wife's left hand as an object, officially starting the history of human beings using X-rays to see through the human body structure. Since then, X-rays have been widely used in the medical field, and CT technology invented based on them has also been widely used in modern clinical medicine.
In this issue, we will take you to understand how CT technology has evolved over more than a hundred years to derive oral
CBCT.
Two-dimensional X-ray imaging to three-dimensional CT imaging
Soon after the discovery of X-rays, scientists began to be dissatisfied with the two-dimensional overlapping images under X-rays, and began to study how to use X-rays to obtain tomographic images without background overlay (called Tomography in English). Research on this goal continued for more than half a century. Finally, in 1972, the British scientist Hounsfield (the unit of CT image value is now named after him, called the "Hounsfield unit") used his own The prototype CT scanned a female patient with a brain tumor and announced his research at the British Annual Meeting of Radiology, announcing the birth of CT (Computed Tomography).
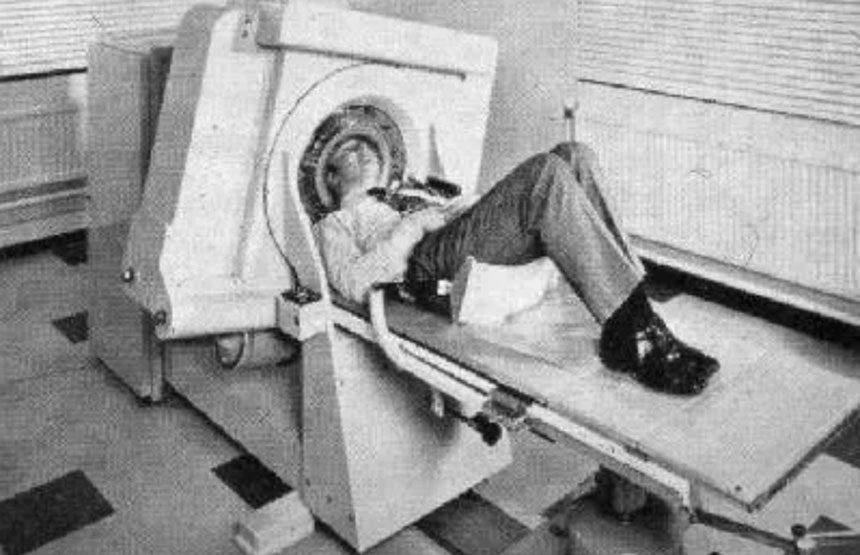
In the next 10-20 years, major companies rushed to join the team of developing CT scanners. The scanning range has expanded from the brain to the whole body, and the image quality has also been significantly improved. However, the basic structure of the system and the technical principles of core components have not fundamentally changed. It was not until 1988 that the world's first Spiral Computed Tomography (Spiral Computed Tomography) was born with the help of slip ring technology. It subverted the scanning method of tomographic CT and became one of the main representative products of CT technology in the following decades.
The original tomographic CT scan requires the patient to remain still and try to avoid movement during the scan. Spiral CT is just the opposite. During the scanning process, the examination table holding the patient is pushed into the scanning hole at a constant speed, and the X-ray tube continuously rotates around the patient, forming a spiral trajectory.
Spiral scanning can obtain information about all tissues within the scanning range, avoiding the disadvantages of easily missing small lesions in tomographic CT scanning. The scanning speed is faster and the imaging is more accurate and clear; its birth is therefore considered a revolution in the development of CT technology. .
"Big image" and "small image", general CT and specialist CT
Before and after the birth of spiral CT, the development of CT technology gradually produced two significant branches, commonly known as "large image" and "small image". Among them, the "large imaging" branch continues to use the traditional CT architecture, that is, a lying examination table and a closed-loop examination hole. By improving the performance of core components, the scanning speed is faster, the scanning volume is larger, and the radiation penetration is stronger, so it can cover the whole body. Including areas such as the heart and head blood vessels that require high imaging speed and low-density contrast. This type of CT is the CT used by most hospital imaging departments in our traditional understanding. Because the images obtained can be used for diagnosis in almost every department, it is also called general CT.
On this development path, multi-slice CT (Multi-slice CT, or Multi-detector CT) was born in the 1990s, which uses multiple rows of detectors and can simultaneously collect multi-slice projection data in a single rotation. The scanning coverage is larger, the scanning time is shortened, and the resolution is higher, resulting in better three-dimensional reconstructed images. Until now, multi-slice spiral CT is still one of the mainstream imaging equipment in the field of medical imaging. After 2000, energy spectrum CT (using fast high-voltage switching light source or double-layer detector technology) and dual-source CT were born. In recent years, photon counting CT has been successfully developed, further improving the resolution of CT images and reducing radiation dose.

Although general CT functions are becoming more and more perfect, they still have fundamental flaws. First of all, the purchase price of tens of millions of yuan makes many small and medium-sized hospitals and clinics prohibitive; secondly, it cannot fully meet the special clinical needs of some departments. For example, due to its closed-loop circular hole structure, general-purpose CT cannot be used for imaging during surgery in the cerebrovascular department; another example is that early breast cancer screening requires an imaging resolution of less than 100 microns. A general-purpose CT that meets this requirement is not only The cost is more expensive, and the radiation dose increases sharply; for another example, the internal structure of the knee joint under weight-bearing conditions can only be obtained when the patient maintains a normal standing posture for imaging, while general CT uses a lying examination table, which cannot complete weight-bearing imaging.
Therefore, in different departments, specialized CT for different lesions or for different clinical applications has developed significantly in the past thirty years. Although they use similar core components, their system structures are flexible and changeable, forming an indispensable and colorful "small image" field.
CBCT and oral CBCT
In order to maintain the flexibility of the machine, specialist CT abandons the classic closed-loop circular hole design in general CT and adopts an open structure. To ensure patient safety, the gantry rotation speed is slow (usually more than 10 seconds per cycle, while the full rotation speed is slow). CT can reach 1 second 4 weeks). In order to ensure that the total time required for data collection does not increase too much, the use of large-area flat-panel detectors becomes a natural choice. Because a large-area flat-panel detector receives an X-ray source and produces a cone-shaped X-ray beam, specialist CT based on flat-panel detectors is also called CBCT (Cone-beam CT).
The Department of Stomatology is one of the earliest departments where CBCT technology has been widely used clinically. Therefore, in the general perception of dental practitioners, CBCT has even become synonymous with oral CBCT. Compared with general CT, oral CBCT has low cost, small size, high resolution, and low radiation dose. Although there are many artifacts and low soft tissue contrast, the image quality is sufficient to meet the clinical needs of oral cavity. Moreover, most CBCT equipment is equipped with independent dental reading software, which has a variety of built-in functions to assist doctors in medical diagnosis, making diagnosis and treatment more professional, and improving the safety and success rate of treatment and surgery.
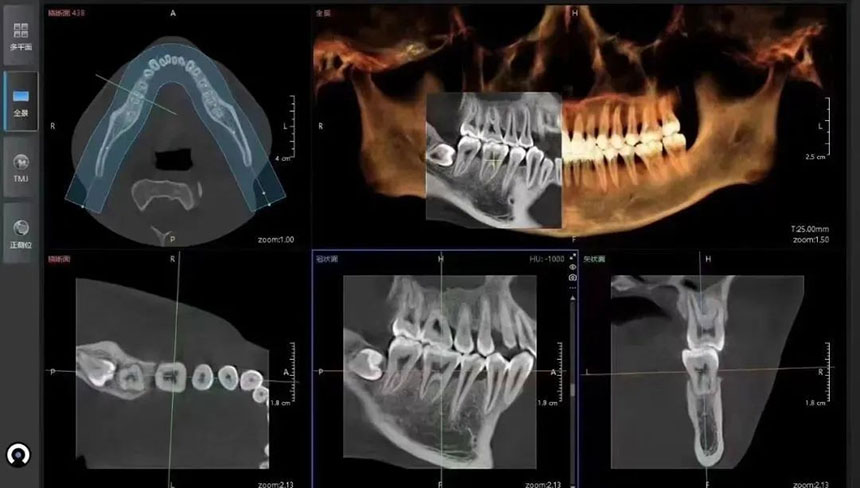
Since the advent of the world's first CBCT in 1995, CBCT has been widely used in the field of oral medicine. Around 2010, CBCT began to enter the Chinese market and quickly gained popularity, becoming the first choice for imaging equipment in most dental institutions. Many large public hospitals that are already equipped with spiral CT have also begun to purchase more practical CBCT equipment. Currently, CBCT has a wide range of clinical applications in the field of oral medicine, including: oral and maxillofacial surgery, periodontal, dental endodontics, orthodontics, implants, etc.
After reading this article, I believe you have a clear understanding of the position of oral CBCT in the entire CT family. Traditional spiral CT is suitable for whole-body scanning, while
CBCT has more advantages and wider clinical applications in the field of oral medicine.








